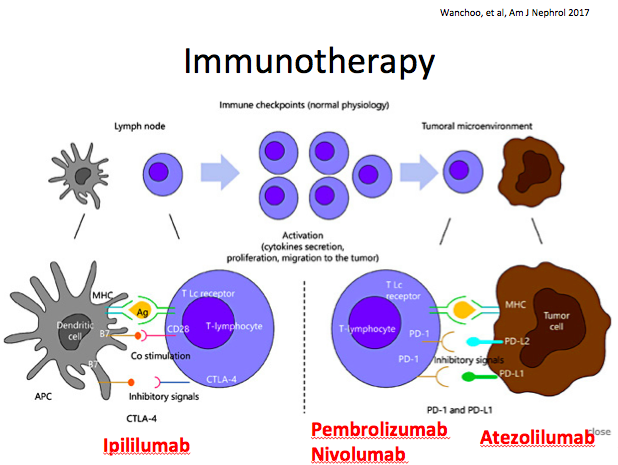
Immunotherapy may also be referred to as “checkpoint inhibitors” because these drugs override the immune system’s mechanisms of restraint to increase recognition and activation of an immune response against tumor cells. A great metaphor is that CTLA-4, PD-1, and PD-L1 inhibitors “take the brakes off,” allowing the immune system to “rev up” to fight cancer .
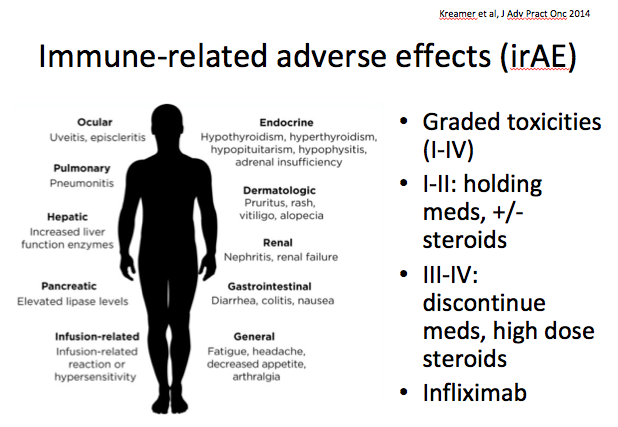
However, as anyone who has ever studied autoimmune disease knows, an overactive immune system can cause damage of its own. Immunotherapy can cause side effects that range from mild to life-threatening in virtually every organ and system; if side effects are severe that is an indication to halt treatment. The decisions on how to manage these toxicities (immune-related adverse effects) are complicated, and while there are guidelines on when/how to treat, the most important part is recognizing a toxicity in the first place–so keep an eye out.
Neulasta and neupogen have similar efficacy for raising the number of neutrophils in the body. However, they are given in different ways.
Neulasta
Neupogen
Generic name
peg-filgrastim
Filgrastim
Tbo-filgrastim (Granix)
Cost
$$$$ Thousands
$$ Hundreds
Mechanism of action
Colony stimulating factor that stimulates production and activation of neutrophils
Colony stimulating factor
Why is it given?
Prevention of chemotherapy-induced neutropenia
Prevention of chemotherapy-induced neutropenia
*Prevention of induction chemotherapy-induced neutropenia in AML, in the setting of bone marrow transplant, and mobilizer for peripheral progenitor blood cell harvesting
How long does it last for?
Half life=15-80 hours (the “Peg-“ recombinant component makes it last longer)
Half life=3-5 hours
How is it given?
Subcutaneous injection >24 hours after last chemotherapy cycle given ONCE
IV infusion or subcutaneous injection given daily to reach target ANC
Adverse effects
Achy muscle or bone pain (ostealgia), rarely capillary leak syndrome, ARDS, glomerulonephritis, hypersensitivity reactions, inducing sickle cell crisis
Also ostealgia, many of the other same adverse effect reported, fever, thrombocytopenia
This refers to one type of renal disease caused by multiple myeloma (MM). MM is a surprisingly common disease, occurring especially in older people, and making up about 10% of hematological malignancies. As you know (or will now learn), MM is a “plasma cell dyscrasia” that results in overproduction of light chains.
According to this excellent summary from JASN, about 50% of MM patients have renal insufficiency at time of diagnosis. The types of kidney injury that can occur range from:
cast nephropathy (common)
light-chain proteinuria (virtually all have proteinuria)
nephrotic syndrome (10-20%)
amyloidosis (5%)
Fanconi syndrome (very rare)
“Myeloma kidney” refers specifically to cast nephropathy. Interestingly, up to 50% of patients initially have their kidney damage attributed to some other cause such as dehydration, infection, hypercalcemia, NSAID injury.
The light chains in MM are usually mutants that can’t be broken down or absorbed the same way that normal light chains are. They form casts in the renal tubules, and because they are “brittle” they can break off and rupture, causing interstitial nephritis. Light chains can also cause direct tubular necrosis, or in rare cases, form “needles” that injure the renal tubules.
Light chain casts (immunofluorescent staining) in the renal tubules. From Korbet and Schwartz, JASN (2006)
Cast nephropathy is pretty serious business. The median survival for someone with cast nephropathy is 36 months, and renal failure is the second-highest cause of death (infection is first).
To treat MM cast nephropathy, it is best to treat the underlying MM with chemotherapy and aggressively manage the creatinine. But, 65% of patients with cast nephropathy will develop end-stage renal disease within 3 months of diagnosis. What to do then?
Another option is dialysis. In some studies, 40% of MM patients with cast nephropathy end up on dialysis and start anywhere from 3 months to a year after diagnosis. However, the effectiveness of dialysis depends on whether the person is responding to chemotherapy, the severity of their kidney disease, and other co-morbidities. Survival can be anywhere from 6 months to 3 years with dialysis, but MM patients still have a 2.5 relative risk of dying compared to other dialysis patients (and remember, these other patients are vasculopaths, severe diabetics, people on the verge of needing a kidney transplant).